
Abilify
By L. Olivier. Wilkes University.
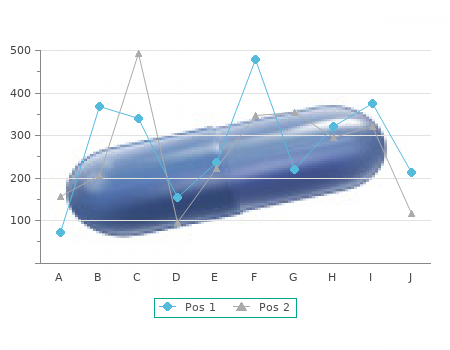
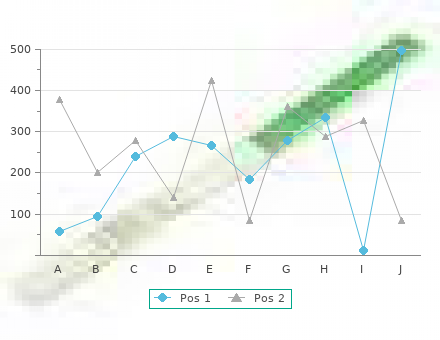
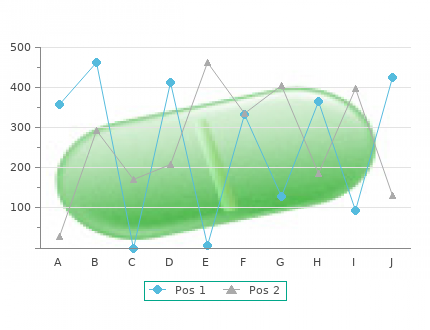
Eight met the eligibility Nonsterile preoperative criteria for fnal inclusion in the systematic urine (2) 8-15 No suitable comparison review cheap 20 mg abilify mastercard. Studies included in qualitative synthesis arm (1) Eight controlled trials randomized a total (n = 12) No suitable outcomes reported (8) of 940 study participants (Table 1) order abilify 20 mg fast delivery. No Guideline recommendations adverse events related to antibiotic prophylaxis were recorded in these studies. Studies of specifc agent for prophylaxis should be based, in part, varied in terms of dose, route and timing of administration on the local epidemiology of drug resistance in potential in the treatment arms. Forest plot of relative risk of urinary tract infection with antibiotic prophylaxis for extracorporeal shock wave lithotripsy. Forest plot of relative risk of fever with antibiotic prophylaxis for extracorporeal shock wave lithotripsy. Results of systematic review Guideline recommendations The literature search identified 1450 citations, and we selected 47 articles for full-text retrieval (Fig. Forest plot of relative risk of urinary tract infection with antibiotic prophylaxis for non- extracorporeal shock wave lithotripsy stone manipulation procedures. Antibiotic prophylaxis for urologic endoscopic procedures excluding Results of the systematic review treatment of renal calculi The 4 trials randomized a total of 2556 study participants Results of literature search (Table 3). Fever involved adults with sterile urine analyses who underwent was not reported as an outcome in any trial. Studies that included participants with positive preopera- The overall quality of evidence was moderate as judged by tive urine cultures were excluded. Antibiotic class We excluded trials that did not report on these outcomes of interest. Fluoroquinolones (1 trial), trimethoprim (1 trial) and ceftri- The literature search identifed 4946 citations, and we axone (1 trial) were studied, and all studies showed a trend selected 140 articles for full-text retrieval (Fig. Forest plot of relative risk of fever with antibiotic prophylaxis for non- extracorporeal shock wave lithotripsy stone manipulation procedures. No adverse events related to antibiotic prophylaxis were recorded in these studies. Results of literature search Antibiotic class Our literature search identifed a recently-published system- atic review of high methodological quality. Results of the systematic review Guideline recommendations The systematic review identifed a total of 28 trials (4694 patients) comparing antibiotics versus placebo. Discussion Records screened Records excluded (n = 6620) (n = 6512) After performing a comprehensive literature Full-text articles excluded review, we have provided executive summa- Full-text articles assessed with reasons (n = 85) ries on the best evidence supporting the use for eligibility (n = 108) of prophylactic antimicrobials in common Not relevant urological procedure (84) urologic procedures. If bacteria are found (n = 4) No suitable comparison arm (3) in the cultures, we strongly recommend pre- No relevant outcomes operative eradication of the infection with a reported (9) Studies included full course of antibiotics according to culture in quantitative synthesis sensitivities. Forest plot of relative risk of urinary tract infection with antibiotic prophylaxis for urologic endoscopic procedures. The overall quality of lit- erature supporting antibiotic use in general was moderate. Antimicrobial prophylaxis for surgery: An advisory statement from the National Surgical Infection Prevention Project. Am In this guideline, it would be remiss not to mention the J Surg 2005;189:395-404. Best practice policy statement on urologic surgery anti- toxicity, such as the development of Clostridium diffcile microbial prophylaxis. Targeted antimicrobial prophylaxis using rectal swab cultures in men undergoing transrectal ultrasound guided prostate biopsy is associated with reduced incidence feedback mechanism, the use of antimicrobial order forms, of postoperative infectious complications and cost of care. Reduction in hospital admission rates due to post-prostate biopsy computerized support. The value of antibiotic prophylaxis during extracorporeal The decision to select a specifc agent for prophylaxis will shock wave lithotripsy in the prevention of urinary tract infections in patients with urine proven sterile be based, in part, on the local epidemiology of drug resis- prior to treatment. Amoxycillin/clavulanate prophylaxis for extracorporeal shock wave that the institutions microbiology/infectious disease team lithotripsy--a comparative study. Antibiotic prophylaxis before extracorporeal shock wave lithotripsy by single-shot application of azlocillin. Antibiotic prophylaxis with enoxacin in extracorporeal shockwave procedural/perioperative course of antimicrobials involving lithotripsy [in German]. Are prophylactic antibiotics necessary during extracorporeal shockwave litho- factors for post-procedural infections may include obesity, tripsy? Antibiotic prophylaxis with aztreonam in patients with kidney extremes of age, nutritional status, diabetes mellitus, immu- 27 stone disease submitted to extracorporeal shock wave lithotripsy. Ann Fr Anesth Reanim1992;11:82- Although these guidelines were created to infuence clinical 7. Antibiotic prophylaxis with cefotaxime in endoscopic extraction of upper urinary tract stones: a the impact of antibiotic use on our medical system and our randomized study. Antibiotic prophylaxis for urodynamic testing in patients with spinal cord injury: A preliminary study.
Part of this reassurance will be provided by screening blood tests such as a complete blood count with platelet count abilify 10mg free shipping. Sigmoidoscopic/colonoscopic examination will rule out most underlying early inflammatory bowel disease and any rectal pathology cheap abilify 20mg, particularly in patients complaining of defecation difficulties or a sensation of being unable to empty the rectum adequately. Following these initial screening tests emphasis should be placed on the stresses present in the patients life, which may trigger their bowel complaints. Evaluating the level of stress and taking steps to correct it will often be helpful. Drug therapy for irritable bowel is usually empiric, directed at the most troublesome symptom (ie. As irritable bowel is a chronic condition and is probably normal for these patients, the chronic use of medications often reinforces the notion that they have a disease. Microscopic Colitis This condition has been recognized increasingly in which the patient with microscopic colitis presents with painless diarrhea. There are two types of microscopic colitis, lymphocytic colitis and collagenous colitis. In collagenous colitis, the basement membrane of the colonic mucosa is thickened by a band of collagen, and in lymphocytic colitis there is an increase in lymphocytes. The natural history of these diseases is unclear and no infective agent has been found. In most patients the disease appears to follow a benign course, but about half of patients continue to have significant diarrhea for more than two years. The symptoms of microscopic colitis are usually controlled by antimotility agents such as loperamide, by use of 5-aminosalicylic acidbased therapies directed at the colon or oral budesonide enteric coated tablets. The most recent studies of therapy have found budesonide (Entocort) to be the most effective therapy. Cholestyramine 4 grams four times a day has also First Principles of Gastroenterology and Hepatology A. Glucocorticoids also control the diarrhea, but in view of the usually benign course of this illness in most patients, steroid therapy should be used only in severely symptomatic patients who cannot be controlled by other therapy. A separate condition, called eosinophilic colitis in which patients with connective tissue disease present with diarrhea of uncertain cause, with negative stool investigations. Like microscopic colitis, the mucosa looks normal on colonoscopy, and the diagnosis is made on mucosal biopsy. All patients initially respond to steroids, but not all patients resolve over time, and some may need prolonged steroid therapy. Because of its lower systemic toxicity, the use of budesonide (as with microscopic colitis) may be the best first line therapy for this rare condition. Therefore, patients with intermittent symptoms are as important to investigate as patients with persistent symptoms, and the story of occasional blood in the stool in a patient over 40 years of age should not be attributed to local anorectal disease without first excluding a more proximal lesion. Presenting features of colon cancer o Abdominal pain, including symptoms of bowel obstruction o Change in bowel habit o Abdominal complaints of recent onset o Rectal bleeding or melena stool o Abdominal mass o Iron deficiency anemia o Hypokalemia Table 2. Patients may not see blood in the stool or note a melena stool, particularly when there is a right-sided colonic lesion. Some patients may present with primarily diarrhea if they have a high output of mucus and fluid from the tumor; in this instance the tumor is often sessile in appearance (see below) and large, with the histology of a villous adenoma. Some patients may have hypokalemia due to the large amounts of mucus secretion from the tumor. Sometimes a search for metastases will reveal a solitary lesion in the liver that may be surgically resectable, or with the early use of chemotherapy, may lead to a cure of the cancer. Polyps of 2 cm or larger have about 50% incidence of cancer, compared to a 1% risk in adenomas less than 1 cm in size. The majority of polyps are completely asymptomatic, but the occurrence of occult bleeding does increase as they grow. Unfortunately, polyps can still be missed, even with occult blood testing of the stool, since the blood loss may be intermittent. Three histologic types of adenomatous polyps occur: tubular, tubulovillous and villous. The malignant potential is greatest in villous polyps (40%) and lowest in tubular polyps (5%), with an intermediate risk in tubulovillous polyps (22%). Polyp snared and ready to transect the stalk of the polyp using electrical current passing through the metal snare wire to completely remove the polyp. The normal tissue of the stalk is seen to the right of the snare in the middle of the image. The base of the resected polyp with the cautery burn evident on the remainder of the stalk. The polyp has been grasped in a Roth net, passed down the operating channel of the colonoscope after the snare is removed and polyp is now removed from the colon to be sent for pathology diagnosis.
For permission to photocopy or use material electronically from this work cheap abilify 15mg on line, please access www buy cheap abilify 20mg line. Trademark Notice: Product or corporate names may be trademarks or registered trademarks, and are used only for identification and explanation without intent to infringe. Foreword When it comes to human nature, there is something about complexity that most people nd troubling. Similar articles inform us that the cause of indelity is purely a product of evolutionary principles, or that a single neurotransmitter is the cause of gambling. As the co-editors of this splendid new volume point out in their preface, psychiatry has not escaped this popular trend toward biological reductionism. The discovery of the genome and the remarkable advances in the neurosciences have fueled the desire to nd discrete causes of complicated human behaviors. Simple biological causes call for simple pharmacologic treatments, and a magic pill is the panacea with which psychiatry is enamored at this historical moment. To a remarkable extent, this reductionist trend within psychiatry as a whole is even more striking when we examine the recent trends in the under- standing and treatment of sexual disorders. The irony, of course, is that no area of human behavior is more mysterious than sexuality. Moreover, if one wanted to conrm the value of the principle of multiple causation in psychiatric disturb- ance, one could do no better than to start with sexual disorders as the prime exem- plar of this principle. As several of the authors in this collection of outstanding contributions point out, approaching the complexities of sexual desire by study- ing problems with genital congestion are likely to produce a limited yield. Balon and Segraves have assembled an international group of experts who share a broad biopsychosocial perspective in their understanding of human sexual dysfunction. To their credit, they in no way give short shrift to biological causes and pharmacologic treatments. Indeed, readers of this book will gain a sophisti- cated understanding of how physiological factors contribute to sexual problems and how to integrate sound medication strategies in their treatments. Going against the grain, it restores a biopsychosocial perspective to the understanding and treatment of sexual dysfunction. It also provides the clinician reader with a practical, commonsense guide to treatment planning that treats the patient as an individual rather than a disease entity. I know of no other text in the eld that can match this state-of-the-art treatment of the subject. Preface The area of treatment of sexual disorders has undergone an enormous expansion during the last few decades. However, the new develop- ments in the area of sexual pharmacology have unfortunately also led to a biological reductionism in the eld. In the present time, physicians in many disciplines view sexual dysfunctions as mostly, if not purely, of biological origin and discard any notion of psychological factors in the etiology of sexual problems. The initial hype about the success rates of sildenal certainly contributed to this notion. However, clinicians who treat sexual dysfunctions/disorders on a daily basis know that in sexual functioning, psychology and biology are intertwined in a very complicated way. In light of that, we feel a text that balances these two not contradictory but complementary etiological views would be highly desirable. A synthesis of biology and psychology in the area of etiology, pathophysiology, and treatment of sexual dysfunction is sorely needed in the eld. We also hope that this text will spark greater interest in the often necess- ary dual approach to treatment of these disorders/dysfunctions among psychia- trists and other specialists. Finally, as psychiatrists who are interested in all aspects of well being of our patients, we hope that this book will help to improve the quality of life and sexual functioning of our patients. Combination Therapy for Sexual Dysfunction: Integrating Sex Therapy and Pharmacotherapy. Faculty of Medicine, McGill University and Department of Obstetrics and Gynecology, Sir Mortimer B. The wide spread usage of effective biological therapies for sexual disorders has contributed to the increasing emphasis on biological models concerning etiology, often to the neglect of psychological factors. In the 1960s, it was commonly assumed that most sexual problems were psychogenic in etiology (1). However, the advent of effective biological therapies has shifted the focus to organic causes of erectile dysfunction (2). These changes in assumed etiology have had profound effects on treatment and conceptualization of the origins of sexual disorders. Many patients who used to be treated by behavioral therapy are now being treated pharmacologically. The rapid development of biological models of therapy has brought valuable help to many individuals who previously had minimal treatment choices. However, a number of factors including the large number of men who dont rell sildenal prescriptions indicate that pharma- cotherapy alone may not always be sufcient (3). To date, there is insufcient data to indicate when pharmacotherapy alone, psychotherapy alone, or combined therapy is indicated for most of the sexual disorders.
Neurogenic : Psychogenic Increased intracranial pressure Acute spinal cord section D safe 10 mg abilify. Drugs and toxins Alcohol Adrenergic medications Consequences of Hypertension (End organ /target organ damage) Patients with hypertension die prematurely buy 10 mg abilify with visa, the most common cause of death is heart disease, with stroke and renal failure also frequent, particularly in patients with retinopathy 1. Effects on the Heart : Left ventricular hypertrophy as a compensatory mechanism Coronary artery disease /Ischemic heart disease: o Angina Pectoris o Myocardial infarction which may lead to heart failure 2. Cerebrovascular disease Transient ischemic attacks : episodic dizziness, unilateral blindness, hemiparesis etc Stroke Ischemic stroke : due to atherosclerosis of cerebral blood vessels 255 Internal Medicine Hemorrhagic stroke: as a result of elevated arterial pressure and formation of vascular micro- aneurysms. Hypertensive encephalopathy: consists of severe hypertension, altered state of consciousness, increased intracranial pressure with papilledema and seizure. Effects on the kidneys : Arteriolosclerosis of the afferent and efferent arterioles and the glumerular capillary tuft impairs renal function. Patients may have proteinuria and microscopic hematuria and later on develop chronic renal failure. Risk factors for an adverse prognosis in hypertension: Black race Youth Male sex Smoking Diabetes mellitus Hypercholesterolemia Obesity Excess alcohol intake Evidence or of end organ damage Approach to a patient with Hypertension: Diagnosis of hypertension: is confirmed after an elevated blood pressure 140/90 mm Hg, properly measured, has been documented on at least 3 separate occasions (based on the average of 2 or more readings taken at each of 2 or more visits after initial screening). Patient evaluation: In evaluating a patient with hypertension the initial history, physical examination and laboratory should be directed at 1) Establishing pretreatment base line hypertension : 2) Identifying correctable secondary caused of hypertension 3) Determining if target organ damage is present: patients may have undiagnosed hypertension for years without having had their blood pressure checked. Therefore, a search for end organ damage should be made through proper history and physical examination. Predisposing factors for hypertension Strong family history of hypertension Age : secondary hypertension often develops before the age of 35 or after 55 Associated cardiovascular risk factors: Cigarette smoking Lipid abnormality or hypercholesterolemia, Diabetes mellitus Family history of early deaths due to cardiovascular diseases Alcoholism. The presence of papilledema and other neurologic signs raises the possibility of increased intracranial pressure Palpation of all peripheral pulses should be performed. These include displacement of apex, a sustained and enlarged apical impulse, and the presence of an S4. Vasodilators: dilate arteriols and arteries, reducing peripheral vascular resistance which inturn reduces high blood pressure. Calcium channel blockers: by modulating calcium release in smooth muscles, calcium channel blockers reduce smooth muscle tone, resulting vasodilatation. In addition they reduce aldosteron production, reducing the retention of sodium and water. Losartan: 25-50 mg once or twice daily Side effects: hypotension 262 Internal Medicine Stepwise prescription of anti-hypertensive medication: Diuretics are often preferred as first line drugs. Most drug combinations, using agents that act by different mechanisms, have an additive effect. Hypertensive crisis: is defined as severe hypertension characterized by diastolic blood pressure greater than 130 mmHg. Blood pressure elevation to such degree can cause vascular damage, encephalopathy, retinal hemorrhage, renal damage and death. In these conditions, the blood pressure should be lowered aggressively over minutes to hours. Pericarditis and Pericardial effusion Learning objectives: at the end of this lesson the student will be able to: 1. Definition: Pericarditis is an inflammation of the pericardium surrounding the heart. Percarditis and cardiac tamponade are clinical problems involving the potential space surrounding the heart or pericardium. Pericarditis is one cause of fluid accumulation in this potential space and cardiac tamponade is the hemodynamic result of fluid accumulation. Pathophysiology: The pericardium consists of an outer fibrous layer (parietal pericardium) and an inner serous layer (visceral pericardium). The pericardium serves as a protective barrier from the spread of infection or inflammation from adjacent structures. It also prevents sudden dilatation of the cardiac chambers during exercise and hypervolumia. It restricts the anatomic position of the heart and minimizes friction with the surrounding structures. Approximately 120 cc of additional fluid can accumulate in the pericardium without an increase in pressure. Further fluid accumulation can result in marked increases in pericardial pressure, eliciting decreased cardiac output and hypotension (cardiac tamponade). Classification of Pericarditis Clinical classification Etiologic Classification I. Clinical features Pericarditis The most common symptom of acute pericarditis is precordial or retrosternal chest pain, usually described as sharp or stabbing. Physical findings: Pericarditis The classic sign of acute pericarditis is pericardial friction rub, which is scratchy, leathery sound heard during both systole and diastole. It is best, heard at the lower left sternal border or apex when the patient is positioned sitting forward.
8 of 10 - Review by L. Olivier
Votes: 295 votes
Total customer reviews: 295