
Fosamax
By N. Ines. Summit University of Louisiana.
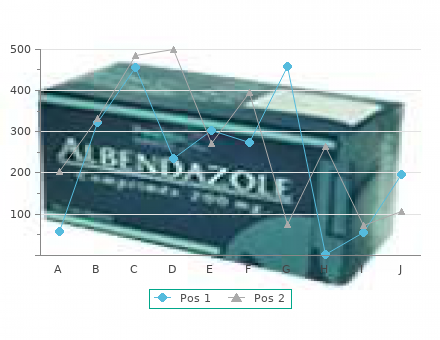
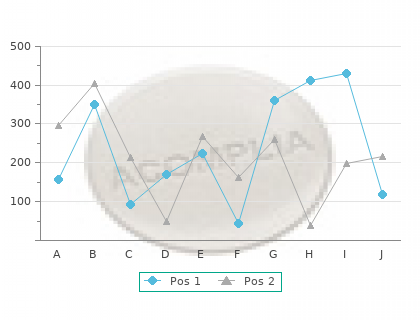
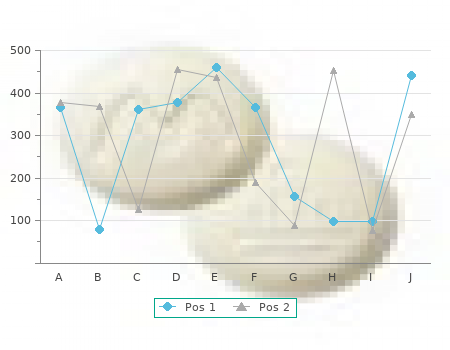
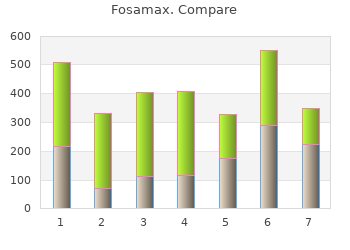
In left panel buy fosamax 35mg without a prescription, drug release from the patch into an aqueous receptor is measured (“Experiment A”) fosamax 70mg without prescription. In the right panel (“Experiment B”) the transport kinetics are re-assessed when excised skin is interposed between the patch and the receiving medium (Modified from Hadgraft J. In the second (Experiment B), drug release into the same aqueous receptor is again measured, but now the skin is interposed between the patch and the receiver medium. If the patch is perfectly rate- controlling, the rates of appearance of drug into the receptor phase in the two experiments will be identical. On the other hand, if the drug arrives more slowly in Experiment B than in Experiment A, it can be concluded that the skin is playing at least some role in controlling the drug’s flux into the body. The results of these experiments for the three nitroglycerin patches are shown in Figure 8. It is immediately apparent that the release of drug from Nitrodur is much greater in the absence of skin than when skin is present (compare nearly 76 mg released in Experiment A in 24 hours with 10 mg released in Experiment B). By contrast, for Deponit, the amounts reaching the receptor phase in 24 hours in Experiments A and B are quite similar, about 11 and 10 mg, respectively. Transderm-Nitro falls in between, with ~22 mg released in Experiment A, compared to 10 mg in Experiment B. However, the differences between the amounts released in Experiment A clearly reveal that the degree to which each patch controls transport across the skin is different. In fact, the Deponit device exerts considerable control over the input rate of nitroglycerin (nearly 90% patch control), whereas Nitrodur lets the natural barrier function of the skin determine drug absorption into the systemic circulation (approximately 90% skin control). For Transderm-Nitro, despite the presence of the so-called “rate-controlling” membrane, the responsibility for metering the delivery is, on average, shared between patch and skin. The maximum rate that nitroglycerin can diffuse across intact human skin is on the order of 20 µg/cm /hr. On the other hand, if a larger surface area is used (say 40 cm ),2 then ratecontrol can be an integral part of the patch such that nitroglycerin is presented to the skin at only 10 µg/cm /hr. In conclusion, it is evident that transdermal delivery is very much determined by the area of contact between patch and skin. Indeed, dose titration with transdermal delivery is achieved not by altering the formulation but rather by adjusting the size of the system (Figure 8. It is also apparent that delivery is not particularly sensitive to the loading of the patch, especially when the input rate is controlled by the skin. The loading does need to be sufficient, however, to ensure that delivery is maintained for the desired period, and to sustain a diffusional driving force. Next, it must be emphasized that the design of the patch does not necessarily guarantee that it will control the overall delivery (for example, the presence of a membrane in a reservoir system does not ensure 100% control by the patch). Thus, drug loading and the mechanism of drug release from a transdermal delivery system are inappropriate measures for bioequivalence assessment. Finally, it is worth noting that the discussion of rate-control as presented is most applicable during the period of what might be termed “steady-state” delivery. In other words, as the patch is applied there are drug molecules waiting at the external surface of the adhesive that become instantaneously available for transport. At the opposite extreme, if a patch remains in contact with the skin for sufficient time that the drug loading is almost completely depleted then, at this point, delivery control is 204 Figure 8. Of course, with almost all the systems presently used, this situation does not arise as the designated application is such that significant amounts of the “payload” remain in the device when it is replaced with a fresh system. However, it is not inconceivable that such depleting systems may become more common in the future, especially for drug substances which are exquisitely potent or expensive or potentially subject to abuse. Scopolamine Scopolamine was the first drug to be marketed as a transdermal delivery system (Transderm-Scop) to alleviate the discomfort of motion sickness. After oral administration, scopolamine has a short duration of action because of a high first-pass effect. In addition, several side-effects are associated with the peak plasma levels obtained. Transderm-Scop is a reservoir system that incorporates two types of release mechanims: a rapid, short-term release of drug from the adhesive layer, superimposed on an essentially zero-order input profile metered by the microporous membrane separating the reservoir from the skin surface. The scopolamine patch is able to maintain plasma levels in the therapeutic window for extended periods of time, delivering 0. Nitroglycerin This drug has been used to treat angina pectoris for over 100 years. It is a potent compound with a high clearance (266 L/hr), short half-life (1–4 minutes) and extremely low oral bioavailability (<1%). Percutaneous transport of mtroglycerin is relatively efficient, and conventional ointment formulations were the first modern-day transdermal formulations available. In the early 1980s, however, three patches appeared more or less simultaneously (Transderm-Nitro NitroDisc, and NitroDur), and transdermal delivery became widely recognized as an alternative route of administration for appropriate drugs. Since that time, numerous new and modified patches have been approved which differ considerably in design, composition, drug loading and release mechanism. Nevertheless, it is possible to demonstrate a bioequivalence between these patches, in terms of the resulting plasma concentration versus time profiles (Figure 8. When nitroglycerin is delivered via the skin, a sustained concentration can be achieved over an extended period of time.
Anoscopy and proctosigmoidoscopy should be deferred until healing occurs or the procedure can be performed under anesthesia buy cheap fosamax 35 mg on line. Eisenstat in the initial evaluation of a patient with a fissure generic fosamax 35 mg on line, they must be per- formed during a subsequent visit because the presence of associated anorectal malignancy or inflammatory bowel disease must be excluded. Ulcers occurring off the midline or away from the mucocutan- eous junction are suspect. Treatment using stool softeners, bulk agents, and sitz baths is suc- cessful in healing 90% of anal fissures. Patients are instructed to soak in a hot bath and contract the sphincters to identify the muscle in spasm and then focus on relaxing that muscle. Botox infiltration into the inter- nal sphincters may be effective in the treatment of anal fissures. Lateral internal sphincterotomy is the procedure of choice for many surgeons after conservative measures have failed. Hemorrhoids Patients with perianal pathology often present or are referred with a chief complaint of “hemorrhoids. Those individuals with painless bleeding due to hemorrhoids must be distinguished from those with bleeding from colorectal malignancy, inflammatory bowel disease, diverticular disease, and adenomatous polyps. Rectal prolapse must be distin- guished from hemorrhoids because it is safe to band a hemorrhoid but not a prolapsed rectum. Hemorrhoidal tissues are part of the normal anatomy of the distal rectum and anal canal. The disease state of “hemorrhoids” exists when the internal complex becomes chronically engorged or the tissue pro- lapses into the anal canal as the result of laxity of the surrounding con- nective tissue and dilatation of the veins. External hemorrhoids may thrombose, leading to acute onset of severe perianal pain. Internal hemorrhoids may have two main pathophysiologic mecha- nisms seen in two distinct but not exclusive groups: older women and younger men. Internal hemorrhoids originate above the dentate line and are lined with insensate rectal columnar and transitional mucosa. In older women, the pathophysiologic mechanism may be related to earlier pregnancy or chronic straining, which leads to vascular engorgement and dilatation, resulting in stretching and disruption of the supporting connective tissue surrounding the vascular channels. Another suggested pathologic mechanism, and the one that may be more important in younger men, is that of increased resting pressures within the anal canal, leading to decreased venous return. Internal hemorrhoids typically do not cause pain but rather bright-red bleed- ing per rectum, mucous discharge, and a sense of rectal fullness or discomfort. External hemorrhoids may develop an acute intravascular thrombus, which is associated with acute onset of extreme perianal pain. Perianal Complaints 475 Grade 1 Rubber banding Internal Repeat as Infrared coagulation Failed needed Determine Grade 2 Sclerotherapy severity Diet changes Failed Initial assessment • History Grade 3 Consider nonsurgical • Exam therapy Failed Surgery • Classification Grade 4 Surgery Thrombectomy, if thrombosed External Improve hygiene Failed Surgery Topical agents Special circumstances • Pregnancy • Inflammatory bowel disease Algorithm 26. Repeated episodes of dilatation and thrombosis may lead to enlargement of the overlying skin, which is seen as a skin tag on physical exam. As in Case 2, the acutely throm- bosed external hemorrhoid is seen as a purplish, edematous, tense sub- cutaneous perianal mass that is quite tender. The complications of internal or external hemorrhoids are the indi- cations for medical or surgical intervention: bleeding, pain, necrosis, mucous discharge, moisture, and, rarely, perianal sepsis. Internal hemorrhoids that fail to respond to medical management may be treated with elastic band ligation, scle- rosis, photocoagulation, cryosurgery, excisional hemorrhoidectomy, and many other local techniques that induce scarring and fixation of the hemorrhoids to the underlying tissues. The acutely thrombosed external hemorrhoid may be treated with excision of the hemorrhoid or clot evacuation if the patient presents within 48 hours of onset of symptoms. If the patient presents more than 48 hours after onset of symptoms, conservation management with warm sitz baths, high-fiber diet, stool softeners, and reassurance is advised. Pilonidal Disease Patients with pilonidal disease may present with small midline pits or an abscess(es) off the midline near the coccyx or sacrum. The workup is limited to a physical exam unless one suspects Crohn’s disease; then 476 S. The differential diag- nosis includes abscess/fistulous disease of the anus, hidradenitis sup- purativa, furuncle, and actinomycosis. For those who fail to heal after 3 months or develop a chronic draining sinus, definitive therapy is recommended. The preferred method is to excise the pilonidal disease and primarily close the defect with rota- tional flaps over closed suction drainage. Neoplasms Historically, the anal canal has been defined as the region above the dentate line, and the anal margin has been defined as the area below the dentate line. Squamous cell tumors of the anal margin are well dif- ferentiated, keratinizing tumors that behave similarly to squamous cell tumors of the skin elsewhere. Tumors of the anal canal are aggressive, high-grade tumors with significant risk for metastasis. Tumors of the Anal Margin Squamous Cell Carcinoma Patients frequently complain of a lump, bleeding, itching, pain, or tenesmus (complaints common to most lesions of this region). Typi- cally, the lesions are large, are centrally ulcerated with rolled everted Table 26. Perianal Complaints 477 edges, and have been present for more than 2 years before detection.
Rinse these thoroughly first order fosamax 35 mg line, throw away shriveled ones order fosamax 35 mg, and add vitamin C to the cooking water. Bala Cuzmin, age 72, had high blood pressure for ten years but the upper (systolic) pressure remained high in spite of various medi- cines that were tried. She stopped using caffeine, switching to arginine tablets to get over the let-down. Her diet was changed to reduce phosphate and add calcium, and she took magnesium and Vitamin B6 to assist the kidneys. She killed parasites, cleansed kidneys but saw no drop in blood pressure which stayed at 150 to 170 systolic. She had all the metal in her mouth replaced and promptly saw a blood pressure drop to 145-1 50. She had phosphate crystals in her kidneys and was started on kidney herbs and a diet change to include milk and exclude soda pop. She was feeling so much better after the kidney cleanse that she decided to remove her last fillings and replace her bridge, too, since it was shedding ruthenium. On her way home from the dentist, her ears stopped ringing and soon her blood pressure was down to 126/68. She was still on half a dose of drugs because she was too afraid to go off entirely. This gave her the energy she wanted to play basketball with the grandchildren again. Then he could cut back on his medicines, measuring his blood pressure daily to guide him. After seven weeks it was down to 140/85, so he decided to do without medicine, a bit early. His next chore, which he approached gladly, was removal of all metal from his mouth. He still had some Ascaris and other health problems but was highly motivated to clean them up, too. Glaucoma In glaucoma the pressure in the eyeball gets too high, putting pressure on fragile retina cells that do your seeing. It is your tip-off, though, that something is not right and you should correct it now, when it is easy, and before other damage is done. Read the section on high blood pressure (page 210) to learn how to reduce it by going off caffeine, checking for cadmium poisoning from your water pipes, and cleansing the kidneys (page 549). Simply getting your blood pressure to normal is sufficient help for beginning glaucoma. Antonia Guerrero, age 51, had glaucoma for five years and was dete- riorating rapidly. She cleansed her kidneys, killed parasites and changed her diet to the anti-arthritic one since she also suffered from arthritis in her hands for ten years with painful enlarged knuckles. She got rid of her asbestos toxins by bringing her own hair blower with her to the hairdresser. After seven months she had pain relief for her arthritis (without aspirin) and her glaucoma was pronounced stable by her ophthalmologist. We must look at the enamel, dentine and root of the tooth as well as the bone they rest in for some answers. Since commerce determines which re- search can be done (that is, paid for) sacred territory can be ig- nored. For example, the effects of sugar-eating, gum-chewing, tooth brushing, fluoridation, tooth filling materials and diet can be ignored if it interferes with product sales. Trivial studies such as comparing shapes of toothbrushes, studying the chemical composition of plaque, and studies of bacterial structure and genes are done instead. His scientific studies stand as a bea- con even today because truths, once found, do not change. He described what he saw in a book, titled Nutrition and Physical 13 Degeneration. Skulls of primitive peoples who lived along coastlines, such as Peruvians, Scandinavians and various islanders, and whose staple foods included fish daily, showed perfect teeth; not a single cavity in a lifetime. Skeletal structure was fully developed, meaning the jaw bone was not undershot or cheek bones squeezed together, forcing the teeth to grow into a smaller than ideal space. Consequently, there was room for the wisdom teeth, and no need to crowd the remainder. The authors estimated a daily consumption of 4 to 5 grams of calcium in their fish containing diet. These primitive peoples got all the calcium, magnesium, phosphate, boron and other bone builders they needed simply from eating (fish) bones. Mexican peoples got 4 to 6 grams of calcium a day from stone-grinding of corn for their staple, tortillas, instead of from fish.
He concurred cheap 35 mg fosamax overnight delivery, after learning about the options order 35mg fosamax mastercard, the procedure, and the significant risks. A preoperative ultrasound study of the neck revealed no abnormality except for a left thyroid lobe solid nodule, 1. Benign Lesions of the Head and Neck Congenital Thyroglossal duct cysts are in the midline, may enlarge quickly with infection, and elevate with tongue protrusion (see Algorithm 11. These lesions are removed completely (including the central portion of the hyoid bone) with general anesthesia. It is important to recognize that this might be the only functional thyroid tissue present; this means that normal thyroid must be identified by scanning technique before any surgical intervention is planned. Dermoid cysts, consisting of elements from all three germ cell layers, are rare in the head and neck. First branchial cleft sinus or cyst presents in the preauricular skin, lying close to the parotid gland. Second branchial cleft cyst presents at the anterior border of the sternocleidomastoid muscle in the middle or lower neck or as a large tender infected mass under the muscle. After treatment of the acute infection, the child or young adult returns for elective surgical removal. A cystic hygroma is a large, soft mass in the side of the neck above the clavicle. These complex, cystic lesions present in infancy and are difficult to remove; suspected cases should be referred to a pediatric surgeon for definitive management. In older patients, the differential diagnosis of a mass presenting in the upper neck must be considered: metastatic cancer, carotid body 186 J. Agnese tumor, carotid artery aneurysm, branchial cleft cyst, or a primary cancer (see Algorithm 11. Salivary gland tumors are most common in the parotid gland, and the majority of these are benign (75–85%). All parotid tumors are removed by surgeons experienced in dissecting parotid tissue off the seventh cranial nerve. In the case of malignant tumors of the parotid, the nerve is no longer sacrificed (unless it is grossly involved with cancer), and the area is treated by irradiation after surgery. Infections In a child or teenager, upper neck masses usually are enlarged lymph nodes draining an infected area. In the posterolateral neck, lateral to the sternocleidomastoid, and in the posterior triangle, these lumps almost always are inflamed nodes draining a zone of scalp infection. A mass in the thyroid or adjacent to the thyroid is relatively common in all ages with the exception of infancy. Scrofula (tuberculous lymphadenitis in the neck) is treated medically after diagnosis has been made. One actually might avoid the usual skin test in this case because the intermediate tuberculin test could result in a huge reaction, with skin slough of the forearm. Ludwig’s angina is a severe, spreading, acute infection that arises from mixed mouth bacterial flora. It involves the floor of the mouth and produces pain and tenderness under the jaw in the midline. Imme- diate referral is essential because some patients require emergency drainage in addition to antibiotics to protect the airway. Vincent’s angina (“trench mouth”) develops from poor hygiene and ulcerations in the gums, and is noted by fetid odor, acute infection, and rapid spreading. Referral usually is indicated, because differentiation from Ludwig’s angina is important. Aneurysms of the carotid artery and a tortuous innominate artery present as pulsatile masses in the lateral neck. While color flow Doppler clarifies these diagnoses, con- sultation with a vascular surgeon should be strongly considered. Head and Neck Lesions 187 Parathyroid The two superior parathyroid glands arise from the fourth branchial pouches, along with the lateral thyroid lobes. The two inferior glands arise from the third branchial pouches and normally lie more anterior than the superior two. This condition can result in bone demineralization, fractures, severe arthritis, renal failure, ureteral stones, acute pancreatitis, peptic ulcer, and mental changes. Since the majority of cases are caused by a single parathyoid adenoma, identification of the site of the adenoma, if possible, allows a more rapid procedure that usually requires only a short stay after surgery. To aid in locating these glands, some use intravenous methylene blue dye preoperatively. To aid locating a single adenoma, one can use a ses- tamibi scan preoperatively and then use a gamma-detecting probe to pick up the radioactive emissions in the operating room.
10 of 10 - Review by N. Ines
Votes: 98 votes
Total customer reviews: 98